Originally published on Pulse, University of Utah Health’s intranet, June 12, 2017, this is a case study about a content audit for the Women’s Health Services website at University of Utah Health.
Content, if you haven’t noticed, is a complex beast. For example, we spend a lot of time focusing on good content, what it is, where we get it from, and how we deploy it. But we spend less time than we ought on considering the outcome we want from the content we curate and post.
A content audit is a tool that allows us to review the content we have and take its pulse. It’s a great benchmarking tool with which to craft and test which content pieces are performing the best and where there might be gaps in the content. If there is important content missing that would benefit our users, a content audit is likely to reveal this.
Goals
For our content audits [at University of Utah Health], we have identified these specific goals:
- Reduce number of website pages with thin or low-performing content
- Combine pages with thin content OR flesh these pages out, depending on website goals
- Archive pages that are out of date, no longer applicable, or very low performing
- Identify areas where we might want to add content
Where to Start
An audit can be as in depth or concise as the site necessitates. You can also tailor the information you collect in the audit to fit your overall site goals. The typical content audit might include these items:
- Analytics
- Page views
- Time on page
- Bounce Rate
- SEO factors
- Meta title & length
- Meta description & length
- H1 heading
- H2 heading
- Subtitles: additional use?
- Word count
- Content type (video, form, text, etc.)
- Contact information
- Images
- Type of image
- Image alt text
- Affiliated documents
- Duplicate content
- Last modified
We determined to add in these additional audit points as particularly applicable to our patient-facing sites:
- Call to action
- Referring physician link included?
- Specialist list included?
- Related MBM specialty?
- Affiliated service line
- Affiliated marketing campaign
- Affiliated research or other programs
- Any additional content
- Patient experience story included?
- Health Feed/Scope inclusion? [U of U Health blog and podcast respectively]
- Related tags to Health Feed/Scope
- Clinical trials inclusion?
- Patient education?
- Vendor library content included?
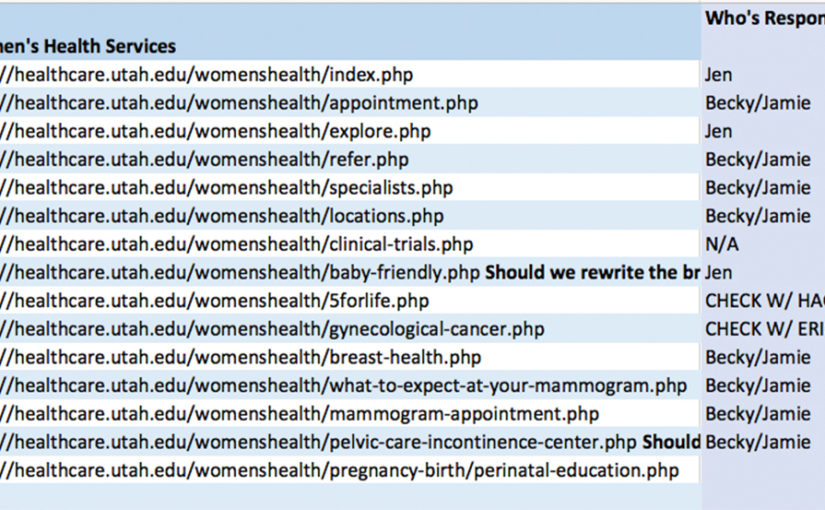
Once you have outlined what you would like to inventory, you can begin to collect the data.* Take a look at the content inventory for our women’s health services website:
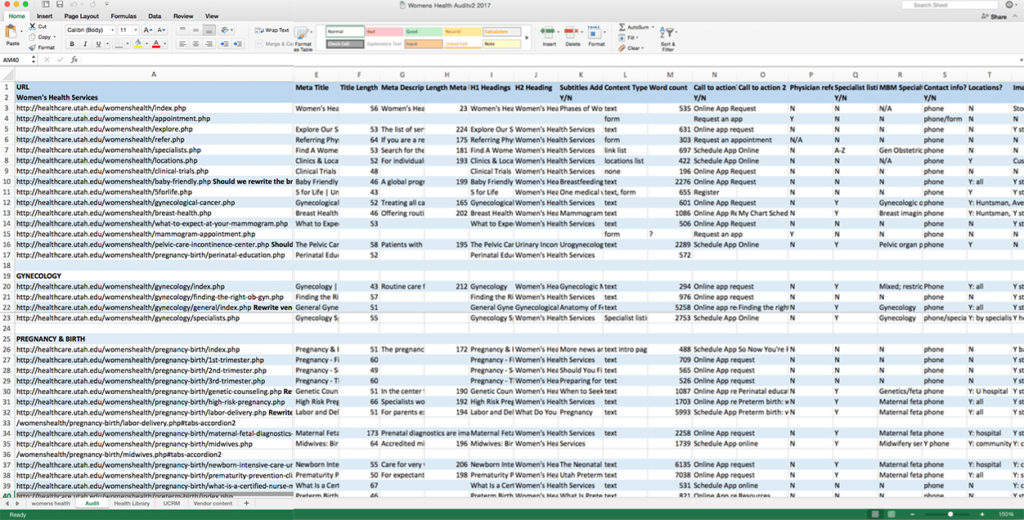
Now that we’ve inventoried the content (rather exhaustively), we can examine how each piece is performing and make some assumptions as to whether the page should be kept, revised, or removed.
Example: Content About Midwives
Previously, we had two website pages about midwives on our women’s health services site. The page /what-is-a-certified-nurse-midwife.php receives far fewer page views than the /midwives.php page. However, this is not necessarily a bad thing, particularly as the time on page is over 1 minute. That’s a lot of time in our virtual ‘verse. So the content is important to those who are looking at it, even though the page doesn’t receive a lot of traffic.
In this case rather than get rid of the content, we are going to optimize it by moving it onto a page with more visibility, in this case /midwives.php. This should increase the main midwife page’s value while indicating to Google that we have both updated our site and checked our content for accuracy. (When search engines crawl websites they look for a number of factors that might tell the importance of the webpage. One of these factors is the date the page was last modified.)
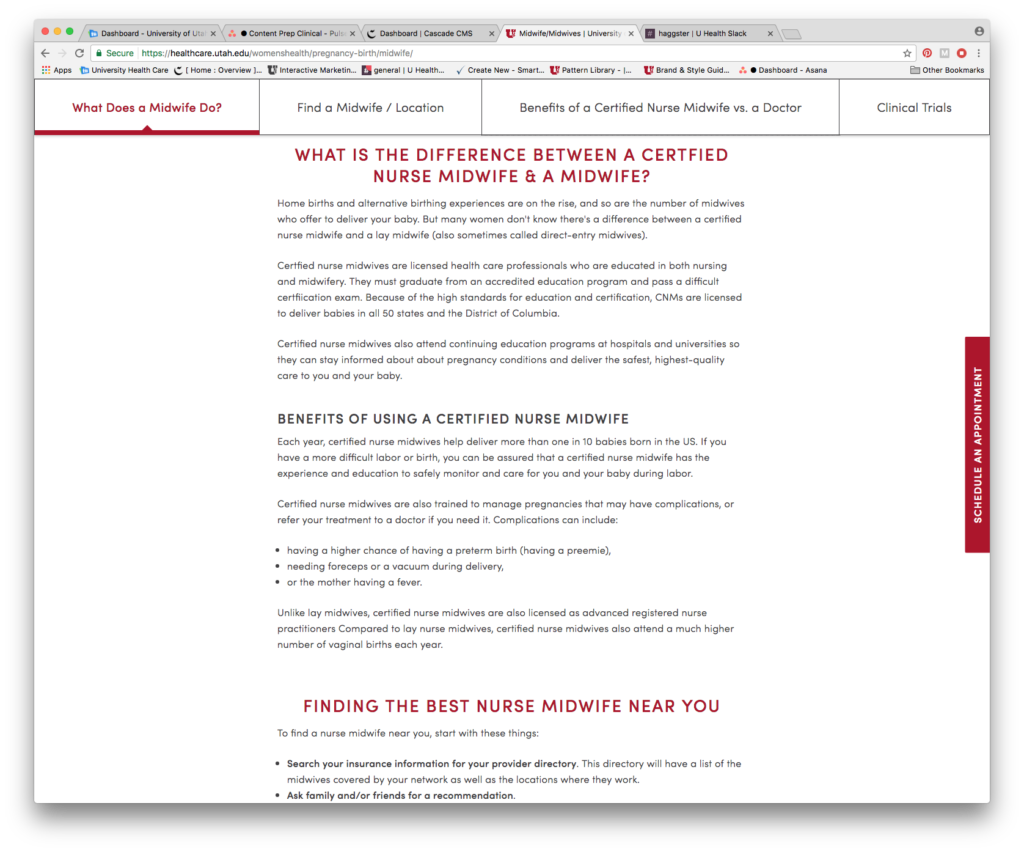
The sticky navigation (a navigation bar stays with you as you scroll down the page) allows readers to access all the content about midwives and our services without leaving this page for another. Thus we’ve consolidated a low-performing, but important, page into the content with which it fits, letting the search engine know that we’ve updated the content by modifying the page, while keeping content that is clearly valuable for our readers.
End Objective: Increase Quality of Page Visits
This is just one page treatment out of many options that we might use when it comes to structuring content. All of the content audit goals lead to the most important objective of our content strategy: increase not just traffic to the website, but the quality of the traffic; namely, we want this content to show up for the right people at the right time in the right place.
Where Do We Go Next?
What happens after an audit? We look at the recommendations we’ve made after reviewing each page and determine who is responsible for whatever action needs to be taken. We also track the progress of the content updates.
Ideally, we apply this process to all our websites on a regular basis, ensuring that our content remains up to date and within best practices.
And that, my friends, is the short of it (the long is all wrapped up in all that data and detail gathering). In the next few months, we’ll keep checking in on this content to see how the website data analytics change (usually we must allow about six months to get a relatively accurate picture of how the content is performing—performance has leveled out by then after the significant changes have been made to the site by then).
*I’m afraid I’ve had to redact the data here; I’m sure you understand!.
